Continue
Glaucoma Drainage Implants are a group of procedures that are the conventional incisional surgeries for glaucoma. These surgeries are indicated for more advanced glaucomas, where the disease is more severe, and the eye pressure is much more difficult to control. Glaucoma drainage implants are often used for secondary glaucomas.
Glaucoma drainage implants are larger devices and require more manipulation to implant. The surgeries take longer to perform than the MIGS procedures, and there is a longer recovery period. However, they are necessary in cases where MIGS procedures will not work.
The risks of post-operative problems are increased with glaucoma drainage implant surgeries, in part, because the eye pressures are usually extremely high to start, and the eyes have more complex glaucoma problems.
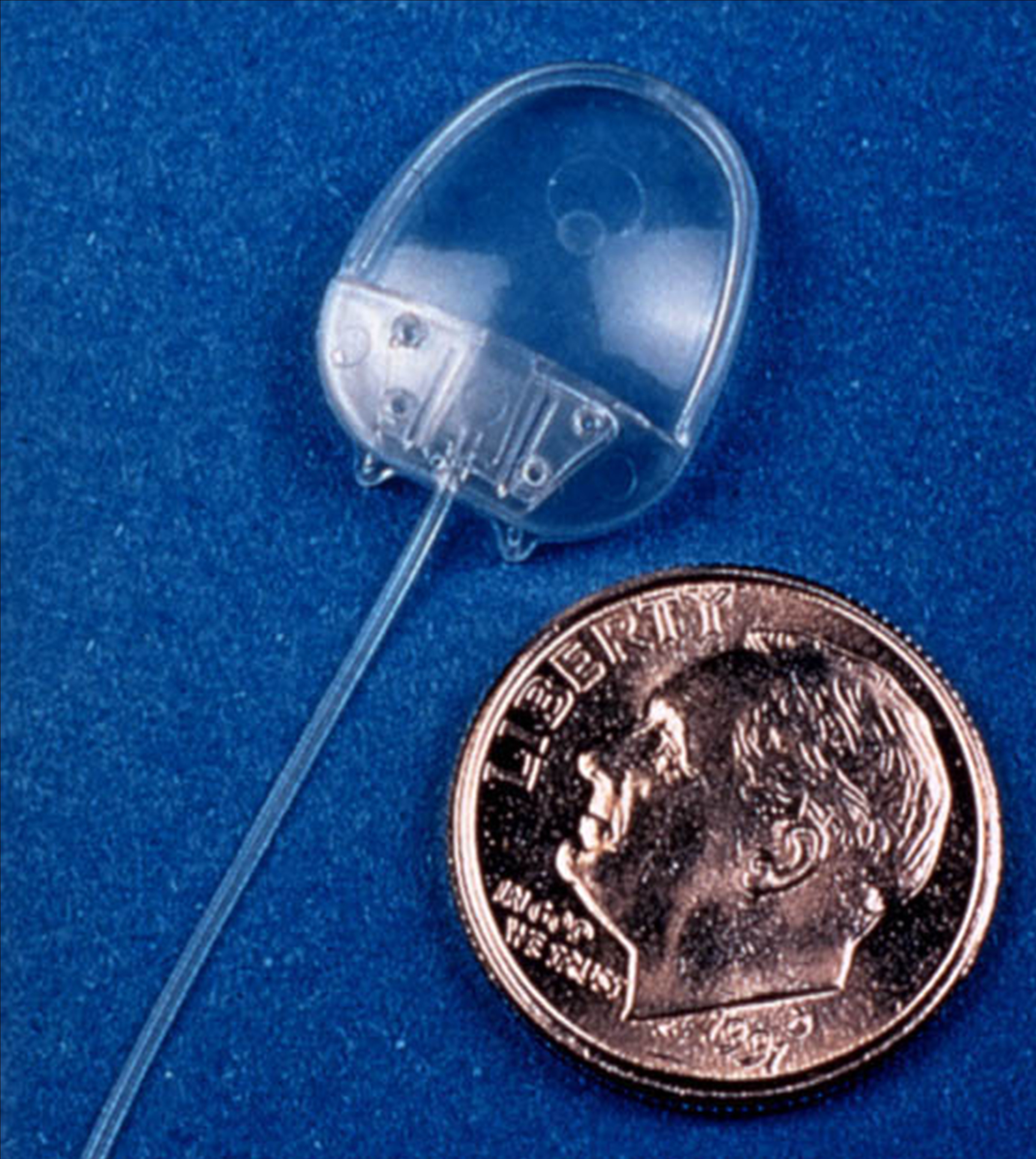
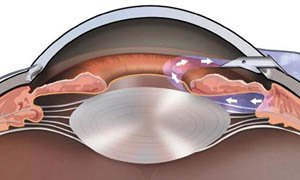
The Ahmed Glaucoma Valve is a commonly used glaucoma implant. The device is composed of plastic and consists of a tube connected to a plate with a valve mechanism. The tube is inserted into the anterior chamber of the eye, and the plate is secured to the eye further back. The tube drains the aqueous fluid out of the eye into a reservoir above the plate. When fully healed, the patient does not feel or see the device in place.
Relative size of the Ahmed Glaucoma Valve
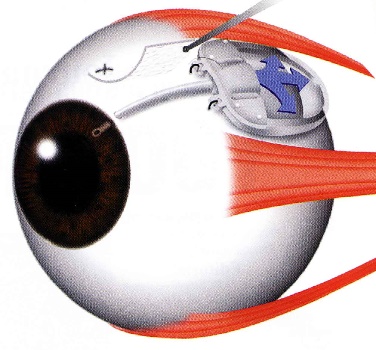
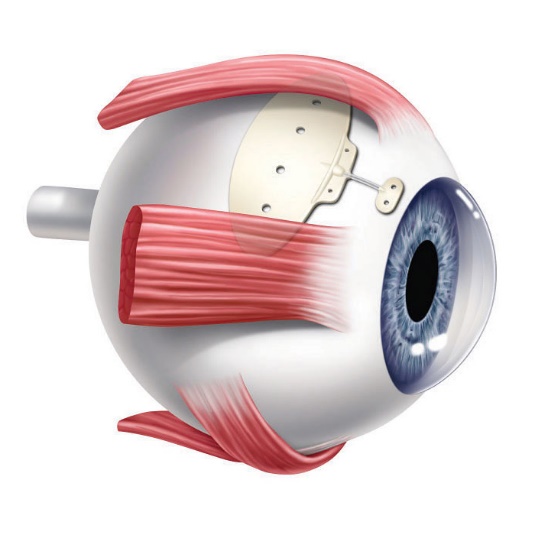
Position of the Ahmed Valve on the Eye
The surgery to place the Ahmed valve usually takes about 45 minutes to perform and is done under local anesthesia. The healing time can take up to a few weeks, but patients can resume most regular activities quickly.
The valve functions to lower the intraocular pressure immediately and is designed to work long-term. Because of the relatively large diameter of the tube, and the position of the plate, the valve is not at high risk for scarring. However, the eye pressure does not always end up as low with the Ahmed valve as with some other glaucoma devices.
The Ahmed valve is preferred when the goal is rapid lowering of intraocular pressure.
The Baerveldt Drainage Implant is the most reliable of all the glaucoma surgeries. It is very effective at achieving low intraocular pressure and is likely to function long-term. The device is composed of plastic and consists of a tube connected to a large plate, but with no valve mechanism. The tube is inserted into the anterior chamber of the eye, and the plate is secured to the eye further back. The tube drains the aqueous out of the eye into a reservoir above the plate. When fully healed, the patient does not feel or see the device in place.
Baerveldt Drainage Implant
Dr. Tesser performing Baerveldt Implant Surgery
The Baerveldt implant surgery takes longer to perform than other glaucoma surgery, and there is usually a longer healing time, up to several weeks, due to its larger size. There is often a delay in the lowering of the eye pressure because the non-valved tube of the device is intentionally tied off with a suture designed to dissolve very slowly. Because of the relatively large diameter of the tube, and the size and position of the plate, the shunt is not at high risk for scarring, and can achieve low eye pressures. The Baerveldt glaucoma implant is best suited for eyes requiring low final eye pressures, and in situations where the other glaucoma devices are likely to fail.
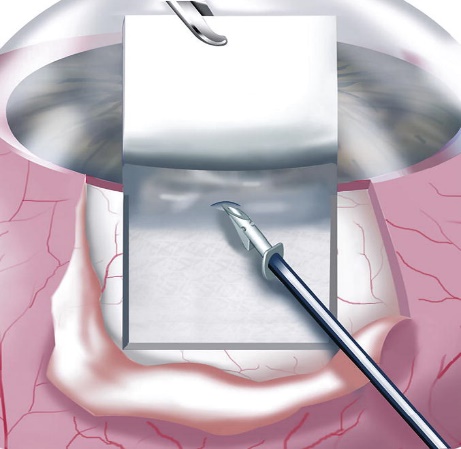
The Ex-Press Mini Shunt is a smaller glaucoma drainage implant device and the surgery, as its names implies, is quicker to perform. The Ex-Press Mini Shunt is a variation of a standard glaucoma operation procedure called a trabeculectomy, often called glaucoma filtration surgery.
The Ex-Press shunt is made of stainless steel. It is a small stent that is placed under a flap of sclera and inserted into the anterior chamber. Aqueous humor fluid flows through the shunt out of the eye into a small reservoir called a bleb. The aqueous is then absorbed by the bleb into the blood circulation of the eye:
Ex-Press Shunt Implantation Under Scleral Flap
Drainage of aqueous humor through the Ex-Press Shunt
The Ex-Press shunt is designed to remain in the eye permanently. It can achieve very low intraocular pressures because the bleb that it creates is often very thin. However, because of its small size it can also stop working due to scar tissue. The Ex-Press Mini Shunt is preferred when the goal of the glaucoma surgery is to achieve the lowest possible pressure.
Cataract and Glaucoma Surgery are often performed together as combined procedures. This is because there is significant overlap between cataracts and glaucoma.
The lens of the eye, because of its position and size, can have significant effects on the fluid flow in the eye, causing the eye pressure to increase. Some glaucoma conditions, such as angle closure glaucoma, are the result of an enlarging cataract.
Some conditions, such as steroid use or diabetes, can cause both cataracts and glaucoma.
Some secondary glaucomas, such as exfoliation glaucoma, are associated with both complex glaucoma and cataracts, each of which more difficult to treat.
As a result, in these and other situations, it is often more efficient to combine the glaucoma and cataract surgeries. The combined surgery can simultaneously achieve both improved vision and a lowering of the eye pressure. In addition, it is more convenient for the patient to have both types of surgery at the same time.
In cases where the glaucoma is mild, and there is a coexisting cataract, combining cataract surgery with a MIGS procedure can reduce or eliminate the number of glaucoma drops that need to be used. In more severe glaucomas, the cataract surgery can be combined with a glaucoma drainage implant.
In certain situations, however, it is best to perform sequential procedures, at different times. This often depends on the relative complexity and severity the cataract or the glaucoma. Either the glaucoma surgery or the cataract surgery can be performed first, followed by the second type of procedure. The time between the procedures can be anywhere from weeks to months, in order to allow the eye to recover form the first procedure.
Make an Appointment